Introduction
Human security is a conceptualization of security and a valuable paradigm for health governance1-5. Criticized for failing to meet a universal consensus on a clear conceptual definition, the concept of human security has transitioned over the last few decades6,7. Most agree that the United Nations Development Programme (UNDP) Global Human Development Report, initiated this evaluation of seven specific elements to comprise human security that include economic security, food security, health security, environmental security, personal security, community security, and political security8-10. Associated often with human rights11, human security has expanded its framework to include non-military threats to community or individual safety9,12, which differs from the traditional approach of security studies for federal or national protection6.
This shift toward an integration of health, structural, political, and environmental factors to overcome inequalities in human populations13is specifically important in developing countries, to decrease vulnerability defined as those features of a social or economic entity that determine the severity of impact likely to be caused by excess morbidity or mortality14. These factors range from biological (eg, individual immunity) to institutional (eg, inadequate health services, access to health care). Moreover, it is important to prevent possible threats under the impact of structural violence, defined as any constraint on human potential caused by economic and political structures15. This form of violence corresponds with the systematic ways in which a given social structure or social institution “harms” people by preventing them from meeting their basic needs. Unequal access to resources, to political power, to education, to health care, or to legal standing, include forms of structural violence15-17.
The Dominican Republic occupies the Eastern two-thirds of Hispaniola island, East of Haiti. Decades of seasonal Haitian immigration to the Dominican Republic provided large populations in agricultural areas, resulting in the formation of Bateyes, isolated rural areas attached to old sugar cane plantations8,18.
These communities have been estimated to include 316 Bateyes, including 230 public Bateyes19 with 43,154 homes and 200,000 residents20. These Bateyes continue to lack central government support to improve the impoverished conditions needed for basic survival20,21 with limited access to hospitals or clinics, basic healthcare, basic hygiene, clean water, and sanitation29,22,23. As the Dominican Republic economy shifted away from sugar cane to tourism, the Batey situation has become increasingly desperate. Infant mortality rates are higher in Bateyes (40 to 45 cases per 1,000 newborns) than in the rest of the country (27 to 31 cases per 1,000 population)24,25, most likely due to respiratory infections, diarrheal diseases, and malnutrition19. Less than 30% of these children receive appropriate immunizations20. The prevalence rate of Human Immunodeficiency Virus (HIV) in Bateyes is almost three times the national rate (2.5% vs. 1%, respec-tively)16, 18, 23, 27-30.
The Dominican Republic has been accused of mistreating Haitians who migrate to specific zones within the country (Bateyes) to work on sugarcane plantations18,21. The impact of this situation, where the treatment identified with this population group has associated external pressures, has motivated the research design, which used principles of the human security model7,16,17 to create an environment of solidarity between Dominicans and Haitians from within the Batey9. The investment in this educational intervention may contribute to reduced acute diarrheal episodes as well as an increased understanding of disease prevention and empathy among community members for resources mobilization and local empowerment. It has the potential to have a beneficial impact on marginalized populations who endure the impact of structural violence. Hence, the purpose of this study was to conduct an economic analysis to evaluate the costs of an educational intervention, using the human security model, and potential sources of economic benefits, in Southwestern Bateyes in the Dominican Republic.
Materials and methods
Study design
Using a quasi-experimental, pre-test, post-test control group design with two study groups (intervention/control), this study aimed to determine the economic impact of an educational program that promoted human security principles, such as environmental, community, and individual security, on disease events (eg, malaria, diarrhea, fever, respiratory diseases), and knowledge (importance of vaccines, HIV-related issues) in the context of elevated HIV prevalence. Through a Rapid Assessment Process (RAP)24, an intensive review of existing data, using a multi-method approach (observation, interviews, literature review) was conducted to obtain information about essential elements of human security in the Southwestern Dominican Republic Bateyes. This included a review of conditions in the Bateyes, including economic security (freedom from poverty), food security (access to food), health security (access to health care and protection from diseases), environmental security (protection from environmental depletion), personal security (physical safety from domestic violence), community security (survival of traditional cultures) and political security (enjoyment of civil and political rights)24. Questionnaires about knowledge, attitude, and practices (KAP) also training materials, obtained from a previous study conducted in a Dominican Republic rural population27and from the World Health Organization (WHO) pamphlets, were used28.
Of over 20 Bateyes located in the Southwestern Dominican Republic, two were randomly selected, which were representative of approximately 10% of the Southwestern sugar mills of the Dominican Republic28. The flip coin method yielded the classification of the intervention group (Batey Algodon, or Batey A) and control group (Batey Altagracia, or Batey B). Both Bateyes share similar poverty living conditions and are 30-45 minutes apart by vehicle. A pilot test was conducted by the Coordinator of Field Activities on the first 15 houses within the selected Bateyes.
Data collection
The project was conducted in three phases and involved a baseline assessment measurement, implementation of the “human security” model for five months, and longitudinal follow-up evaluations of the intervention at six and twelve months. The heads of the households, defined as an individual who spent the previous four nights in the house with no other residence, within the two selected Bateyes were recruited by the Community Workers. Six Community Visitors (two males and four females), or three per Batey, were selected as trained interventionists. Batey A (n = 60 families or 330 individuals) and Batey B (n = 210 families or 1170 individuals) households were assessed at baseline and followed longitudinally with six-month and twelve-month evaluations. Batey A additionally received monthly household visits by a Community Visitor during the subsequent six months. The study was approved by the Institutional Review Boards of the National Research Center for Maternal and Child Health (CENISMI) (the Dominican Republic and the University of Miami (the United States of America. Study participants provided informed consent prior to their study participation.
At the baseline visit, a 45-minute face-to-face structured interview in Spanish or Creole based on the subject’s preference was conducted at the participant’s home by community visitors. Interviewers assessed demographic (age, number of household members, income, gender, and pregnancy status) and environmental characteristics (trash collection, source of water, type of toilet), presence of morbid events (diarrhea, fever, respiratory diseases), past history of infectious diseases (tuberculosis, dengue, malaria, HIV) morbidity and mortality data, geographic mobility, access to medical care and HIV testing. They also held one-hour sessions with families to discuss HIV-related issues (prevention, treatment, stigma, solidarity).
Following the baseline visit, the community workers administered monthly face-to-face sessions with the families in Batey A. These one-hour sessions were conducted within the first five months of the project and the trained interventionist approached the family to talk about HIV-related issues prevention, treatment, stigma, and solidarity. After the HIV information session, the interventionist trained the family in food preparation, water sanitation, breastfeeding, vaccine administration, and infectious diseases prevention, namely diarrhea (water sanitation, use of latrines), respiratory infections (environmental education), HIV (condom use/ accessibility), malaria (bed nets), dengue (covering water tanks with lid, use of Clorox), and tuberculosis (persistent cough for two weeks).
Data analysis
Data were analyzed using NCSS/PASS 2000 and SPSS version 12.5 for Windows. Descriptive statistics were used to calculate the rates and describe demographic characteristics and clinical manifestations. Relative risks and 95% confidence intervals (95% CI) were computed, and Chi-square and Fisher exact tests were used. Associations between structural factors included in the survey and vulnerability of the study unit (Batey) to infectious diseases, as measured by awareness, attitudes, and practices toward infectious diseases, were assessed using bivariate tabulations and calculations of relative risks. Secondary data (eg, census data, Demographic Health Surveys) were used to compare and evaluate the information collected on structural intermediate-level and macro-level factors. Alpha level was set at 0.05. Monthly and quarterly data reports were reviewed for outliers, quality control matches, adherence to protocol accuracy, and consistency with previous reports.
Results
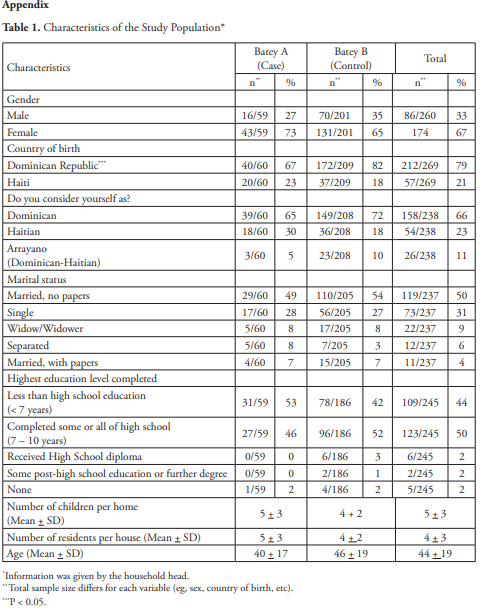
Batey A and B households were visited between September 24 and October 22, 2007. Table 1 presents results from the demographic portion of the questionnaire. The majority of respondents were female (67%), born and raised in the Dominican Republic (79%), and perceived themselves as Dominicans (66%). Characteristics of the families by marital status, level of education, number of children per home, number of residents per house, and age of the head of household indicate similar distribution among Bateyes A and B. Adherence rates ranged from 78% to 100% for monthly visits, and six- and twelve-month follow-up visits to households.
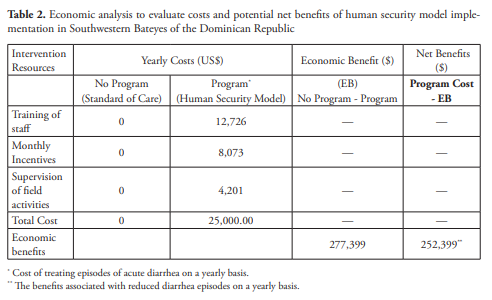
Preliminary data on resource utilization and costs were collected to establish a foundation for examining the economic impact of the program. Costs included: training of study staff (US$12,726), supervision of field activities (US$4,201), and study personnel monthly incentives (US$8,073). In addition, specific outcome measures were identified that could be used to estimate the economic benefits of the program. These measures included: prevention of morbid events for infectious diseases and HIV- related mortality. Program costs and economic benefits were compared across each alternative (Program vs. No program) to estimate net economic benefits (i.e, economic benefits minus costs). Net benefits express the “cost saving” to the Ministry of Health and society overall associated with the Program.
Table 2 presents the results of the cost analysis and potential economic benefits from reducing morbidity (i.e. diarrhea). Intervention resources for the program included staff training, monthly incentive payments to run the intervention, and supervision of field activities. Costs of the intervention were 50% lower than the total cost currently spent by the Dominican Government in infectious disease prevention programs in urban areas of the country. The total yearly cost of the intervention was estimated to be US$25,000. This translates to roughly US$23.00 per Batey resident.
In terms of potential sources of economic benefits, effective treatment for severe acute diarrhea was chosen given its high prevalence in the Bateyes. It is estimated that 50% (n = 675) of the current population of the two selected Bateyes will have at least one episode of diarrhea per year25. Treatment cost for acute diarrhea disease is estimated at US$4571* a burden that falls on the Dominican government. Thus, for each case avoided, the Dominican government would save US$457. Given the potential for disease reduction shown by the intervention (10% of the individuals reported to have diarrhea at the follow-up visits), the benefits associated with reduced diarrhea on an annual basis, would translate to approximately US$277,399 [(675- 68) x 457] dollars for preventing morbid events (i.e. diarrhea). This suggests that by investing $25,000 a year to run the intervention, the net economic benefits would be US$252,399 dollars (Table 2).
If other outcomes are factored in, such as reduced HIV transmission, the potential economic benefits are considerably higher. For example, the WHO estimates that the average cost per case of AIDS is about 2.7 times the per capita GDP29. For the Dominican Republic, this value would be approximately US$23,760 (US$8,800 times 2.7). Thus, if the intervention prevented just 2 cases of HIV/ AIDS per year, the monetary savings would be US$47,520. In addition to the economic savings, there is also a potential economic gain because of the contribution that those prevented cases could make to society. The total net benefits ($47,520 - $25,000) would be $22,520 (from HIV/AIDS prevention only).
Discussion and conclusions
In this study, an educational program, incorporating comprehensive human security principles, such as environmental, community, and individual security (eg, solidarity between Haitians and Dominicans working together to reduce health inequalities), was developed to determine whether health entities (disease events) could be decreased and better health practices (eg, immunization, exclusive breastfeeding) promoted in vulnerable communities living in rural areas (Bateyes) of the Dominican Republic. This case study applied the human security principles to two vulnerable, yet demographically similar, Dominican Republic Batey communities characterized by impoverished living conditions, high HIV prevalence, and increased infant mortality due to other infectious diseases. Examining the economic impact of a human security model versus non-intervention (standard care) on health-related outcomes over time, model implementation demonstrated that the intervention is effective in preventing morbid events.
The model was implemented in Dominican Republic Bateyes, vulnerable communities known for human rights violations and structural violence. As indicated in baseline characteristics of the study population, most participants classified themselves as Dominican, although without rights of residency status. For this reason, this situation calls for the implementation of a human security model that would promote solidarity between family members based on positive interactions between family members and community visitors. These interactions predict the development of sustainable relations between community visitors and Ministry of Health Research Supervisors.
Moreover, the implementation of the human security model demonstrated the feasibility that community visitors, who live in the communities, were able to train families of their communities in prevention methods. Of equal significance, the community visitors were able to work side-by-side with people from the Dominican Republic Government, thereby being available to provide potential solutions to human security issues that could develop in the Southwestern Bateyes of the Dominican Republic.
The economic analysis revealed that cost saving to the Ministry of Health and society overall associated with reducing diarrhea under the program was US$252,399 per year. In this context, if cost saving is extrapolated to the 300 Bateyes of the Dominican Republic, the Dominican Republic Government could save approximately US$75 million in infectious disease prevention by implementing the model in these isolated rural areas of the country. Furthermore, as the analysis was performed for one disease, the projected cost saving would be more because the intervention has the potential to impact on the course of many diseases. However, these costs might be different if this intervention were run directly by the Ministry of Health since the current cost for disease prevention in urban areas of the Dominican Republic is two times higher than the cost of implementing the human security model proposed for this study. Thus, this intervention has also shown that by working with local community members directly, the Ministry of Health could save resources and efficiently address disease prevention and other causes.
Although a formal sensitivity analysis was not conducted to examine changes in cost and outcome parameters, even if we assume the program is only half as effective in other Bateyes, the savings would still be more than US$30 million per year. This preliminary economic analysis provides strong motivation for formally examining the costs and benefits of the human security model in future studies. This type of intervention, however, should be considered as an educational human security model that goes beyond obtaining risks for comparing human populations. The model provides a way to integrate community mechanisms and governmental solidarity, through the interaction of the Community Interventionists with the owners of the houses and with the supervisors from the Ministry of Health, to ultimately reduce social and health inequalities in the Bateyes of the Dominican Republic.
As a human security educational model, which attempts to use human security issues to integrate other essential elements of the human security concept, some limitations need to be acknowledged. Since structural, cultural, and political interventions assessments, which are important aspects of a human security model, were not performed, specific outcomes regarding those factors should be obtained indirectly from qualitative assessments. In fact, a qualitative component should be part of an educational human security model and should be included in future studies that intend to replicate this case study methodology. Another potential study limitation was the statistical differences in KAP observed at baseline between cases and controls. The fact that most of the statistical differences observed at baseline were absent at twelve months post-intervention may have overemphasized the benefits of the model in the case group.
This is the first study on human security implemented in the Dominican Republic. Execution of the model was performed to identify human security factors in vulnerable populations such as the Southwestern Bateyes in the Dominican Republic. The feasibility of the model, implemented by community visitors living in the Bateyes, and their interaction with families and research supervisors of the Dominican Republic Government, demonstrates an important strategy that could be used to obtain international and local resources to support human security approaches in the Bateyes. The final goal was to create a common cause for Dominicans and Haitians to establish a harmonic model of cooperation from the heart of the Bateyes that addresses not only the elimination of structural violence but also the vulnerability still in place in this Southwestern region of the Dominican Republic. Applied to other settings, study design and outcomes could have a beneficial impact on refugee and undocumented populations in other countries under the impact of structural violence observed in the Bateyes.
Funding: This research was economically and technically supported by the Fogarty International Research and Training Program of the University of Miami and Global Strategies for HIV Prevention, California, USA. Study sponsors had no role in the study design, collection, analysis, or manuscript preparation or submission.